
Case-Report | DOI: https://doi.org/10.31579/2578-8868/053
1 Resident, MS Neurosurgery, Department of Neurosurgery, Bangabandhu Sheikh Mujib Medical University. Bangladesh
2 Professor, Department of Neurosurgery, Bangabandhu Sheikh Mujib University. Bangladesh
3 Associate Professor, Department of neurosurgery, Bangabandhu Sheikh Mujib Medical University. Bangladesh
*Corresponding Author: Bipin chaurasia, Study undertaken in the Department of Neurosurgery, Bangabandhu Sheikh Mujib Medical University. Bangladesh
Citation: Chaurasia B, Jahan N, Mosharef Hossain ATM, Bhattachariya R, Barua KK, Halder K, and KM Tarikul Islam. Plasmacytoma of Skull Mimicking Meningioma and Metastasis J. Neuroscience and Neurological Surgery 3(3): DOI:10.31579/2578-8868/053.
Copyright: © 2019 Bipin chaurasia. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 May 2019 | Accepted: 24 June 2019 | Published: 03 July 2019
Keywords: plasmacytoma; meningioma; metastasis;
Plasmacytoma is a tumor arising from plasma cell, which mainly grows within soft tissue or within axial skeleton. When it is present as a discreet solitary mass it is called as solitary plasmacytoma and it is rare. We report a case of 46 years male presented to us with the complaints of painless swelling in the left front parietal region which is about 8.6x6.5cm in diameter .Magnetic resonance imaging(MRI) revealed an extra axial mass in fronto parietal region with overlying bone destruction mimicking meningioma with bony erosion. We did fronto parietal craniectomy and complete resection of tumor with bone margin subsequent cranioplasty also done.Histopathology of which revealed plasmacytoma. After that we did urinary bence jones protein which was negative.
Plasmacytoma is malignant proliferation of plasma cell, mainly arise from proliferation of a single clone of B lymphocyte 3% of which present as solitary lesion [1]. The international myeloma working group lists three types of plasmacytoma: solitary plasmacytoma of bones, extramedullary plasmacytoma & multiple plasmacytoma. Solitary plasmacytoma occurs as lytic lesion. An osteolytic plasmacytoma lesion in skull with no systemic involvement is extremely rare.[2] Multiple myeloma, extramedullary plasmacytoma and solitary bone plasmacytoma all are the three subgroup of plasma cell tumor.[3]
We present a case of plasmacytoma present in frontoparietal region
Case report
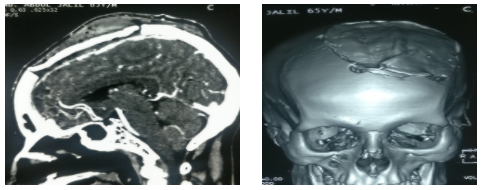
A 77 years male admitted to our department with complaints of gradual enlargement of a painless swelling on his vertex for one year. On examination we found a painless mass in left frontoparietal region measuring about 8.5 x 6.4 cm in diameter which was firm in consistency, not mobile, fixed with underlying & overlying structure, on general physical examination no other abnormality detected, neurological examination was also normal. He has no significant past medical or surgical illness. On MRI of brain revealed a iso to hypointense extra axial lesion involving the left frontoparietal region measuring about 8 x 6 cm causing mass effect over the brain parenchyma (Figure 1, 2, 3, 4).

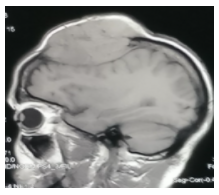
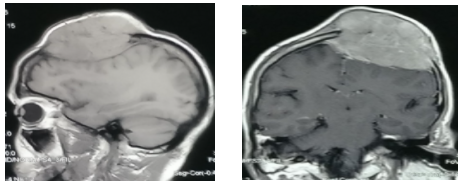
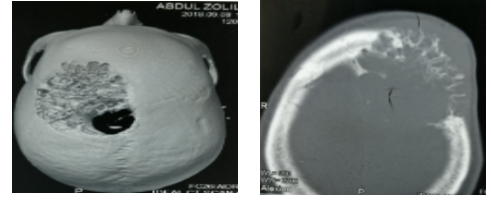
After Intravenous gadolinium showed strong enhancement of the lesion. On CT scan of brain revealed there is a lytic lesion in left frontoparietal region causing a bone defect (Figure.5, 6).
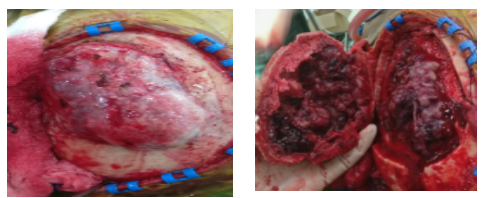
On magnetic resonance venogram displayed the superior sagittal sinus is compressed by the tumor. complete blood count all are within normal range.as our initial diagnosis was may be a case of meningioma or metastasis so we did all metastatic work up eg.thyroid scan, Ultrasonography of whole abdomen and tumor marker but all were normal, He underwent craniectomy peroperative tumor was found to involve the subcutaneous tissue to bone upto dura & which was completely extradural, tumor was moderately vascular, total removal of tumor with involved bone was removed (Figure 7,8).
cranioplasty was done with bone cement (Figure 9,10).
Histopathology revealed plasmacytoma .his post-operative period was uneventful, as there was no other site of lytic lesion and we removed tumor in en bloc with part of dura so radiotherapy was not performed.
Discusson
Plasma cell tumor are divided in three type solitary plasmacytoma of bone (SPB), extramedullary plasmacytoma & multiple myeloma. Multiple myeloma is systemic disease which involved multiple osteolytic lesions, atypical plasma cell in biopsy , amyloid deposit & abnormalities in immunoglobulin production, and the others are local form of plasma cell tumor , According to Bataille and Sany, the diagnostic criteria for SPB include an isolated tumor composed of malignant plasma cells; absence of other lesions on skeletal radiographic survey; absence of plasmacytosis in the bone marrow, absence of anemia, hypercalcemia, or renal involvement & the Vertebrae and pelvic bones are mostly involved by SPB.[3] Solitary plasmacytoma of skull is rare disease and considered to be curable with resection & radiotherapy.[4] Due to its rarity most of the time preoperatively it is misdiagnosed as meningioma or metastasis . As compared to SPB the prognosis of solitary plasmacytoma of skull is good if it is diagnosed on strict criteria. [1] so making the appropriate diagnosis is necessary for further management & follow up, though from some literature they think that solitary plasmacytoma is the initial presentation of multiple myeloma with progression of time this may convert into multiple myeloma. [5]
We went through published literature [ Table:1(4,6-12)] of patients diagnosed as a case of solitary plasmacytoma of skull received en bloc removal of tumor including cranioplasty.

All of those patients are histopathologically proven plasmacytoma of skull among them four patients receive only surgery, no post-operative radiotherapy or chemotherapy, and four patients received surgery along with post-operative radiotherapy, and on follow up among them seven patient has no recurrence except one patient whom post-operative follow up is not available.
Radiotherapy is the definitive treatment for solitary plasmacytoma of bone, surgery along with radiotherapy is the treatment of choice based on tumor location and type of removal of tumor, chemotherapy is not needed until there is systemic involvement as like multiple myeloma. [4] if there is gross total resection of tumor in case of isolated local tumor radiotherapy is needed or not is still in quarry, but as sometimes solitary plasmacytoma is the initial presentation of multiple myeloma regular follow up is necessary in all cases.
Conclusion
Isolated solitary plasmacytoma is a very rare tumor,en bloc tumor removal with removal of involved bone up to macroscopic healthy margin with cranioplasty is a treatment option but as radiotherapy is another option so regular follow up should be carried out.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
